
The Radiologist Shortage Crisis: Why AI as a Second Reader Isn’t Optional Anymore
There aren’t enough radiologists. There won’t be enough radiologists. And the gap between the number of scans that need reading and the number of eyes available to read them is widening every year.
If you’re a radiologist, you already know this. You feel it in the stack of studies waiting when you sit down in the morning. You feel it in the pressure to read faster, work longer, and cover more shifts. You feel it in the Sunday night dread before another week of 60+ cases per day.
The question isn’t whether radiology has a workforce problem. The question is what we do about it while we wait for a generation of trainees that may never fully arrive.
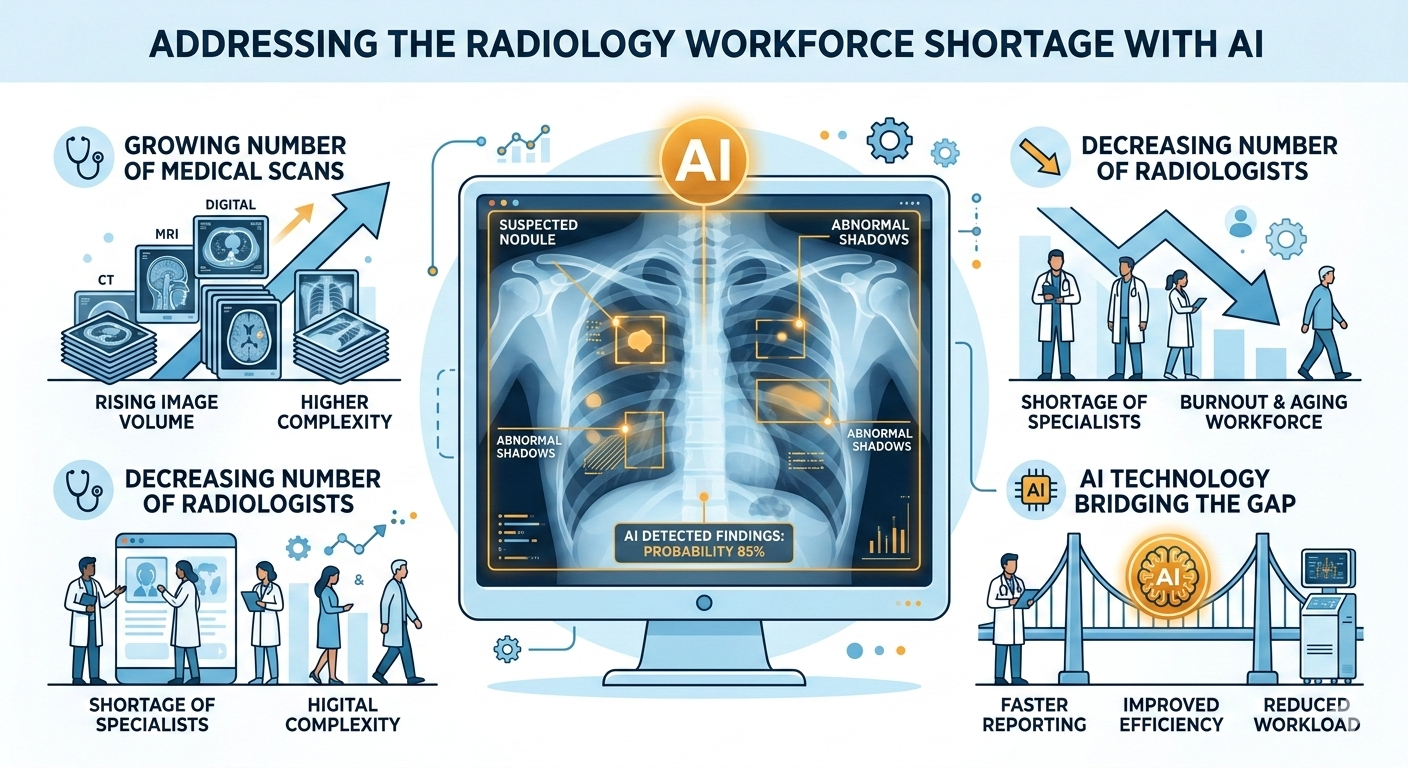
The numbers are stark
The Association of University Radiologists and the American College of Radiology have been tracking this for years. The projections are consistent and grim:
- 19,500 unfilled radiology positions in the United States by 2034, according to workforce modeling from the ACR.
- 3-5% annual growth in imaging volume, driven by aging populations, expanded screening guidelines, and the shift toward image-guided interventions.
- A flat training pipeline. Radiology residency positions have grown modestly, but not nearly enough to match demand. And not every graduate stays in diagnostic radiology — many move into interventional subspecialties or leave clinical practice entirely.
The math doesn’t work. Imaging volume is compounding. The radiologist supply is not.
This isn’t a US-only problem. The UK’s Royal College of Radiologists estimates a 33% shortfall in the clinical radiology workforce. India has roughly one radiologist per 100,000 people. Sub-Saharan Africa has even fewer. Globally, billions of people live in regions where there simply aren’t enough trained eyes to read the scans being produced.
What the shortage actually looks like
Statistics are abstractions. Here’s what the shortage looks like in practice:
Longer turnaround times. A community hospital that once reported chest X-rays in two hours now takes six. The emergency department waits. The patient waits. The referring physician waits. Decisions that depend on imaging findings get delayed.
Coverage gaps. A four-radiologist group loses one member to retirement. The remaining three absorb the volume. They can’t recruit a replacement because the candidate pool is shallow and the salary expectations exceed the group’s revenue model. Nighttime and weekend coverage becomes a rotation of exhausted physicians reading from home.
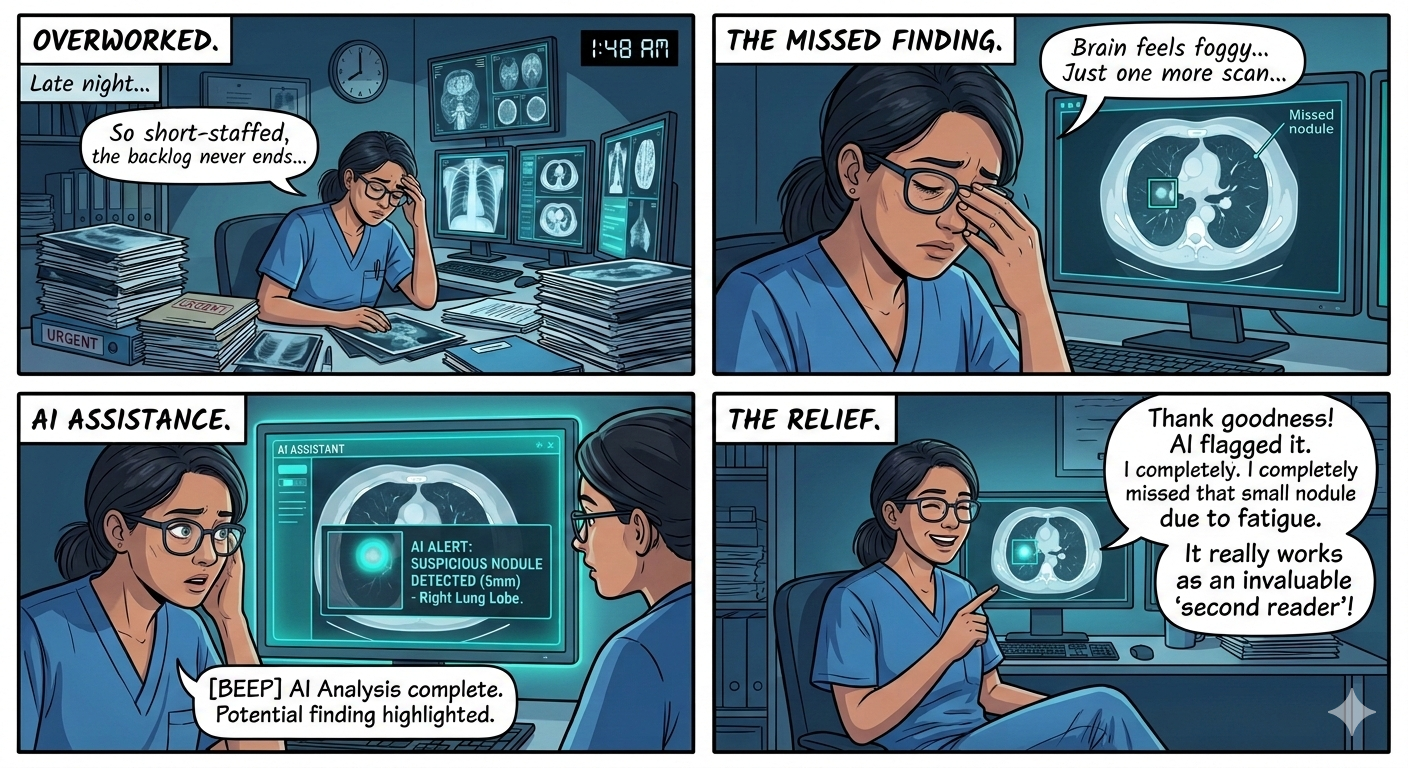
Fatigue-related errors. This is the part that keeps radiologists up at night. Study after study has demonstrated that diagnostic accuracy degrades with volume and fatigue. A 2023 meta-analysis in Radiology found that error rates increase measurably after four continuous hours of reading. A retrospective study in Academic Radiology showed that cases read in the final two hours of an eight-hour shift had a statistically significant increase in missed findings compared to the first two hours.
Radiologists don’t miss findings because they’re careless. They miss findings because they’re human, and they’re being asked to sustain a level of vigilance across hundreds of cases per day that no human cognitive system was designed for.
Burnout. The 2024 ACR survey found that over 50% of practicing radiologists report symptoms of burnout. Not dissatisfaction — burnout. Emotional exhaustion, depersonalization, and a diminished sense of accomplishment. The kind of burnout that leads people to reduce their hours, leave practice, or retire early. Which, of course, makes the shortage worse.
The traditional solutions aren’t scaling
The usual responses to the shortage are well-intentioned but insufficient:
Train more radiologists. We should. We are, modestly. But training a radiologist takes 13 years after high school (4 years college, 4 years medical school, 5 years residency, plus fellowship). Even an aggressive expansion of training positions today won’t produce practicing radiologists until the mid-2030s. And those new graduates will enter a workforce where imaging volume has grown another 30-50% in the interim.
Teleradiology. Remote reading has helped redistribute work geographically. A radiologist in Bangalore can read overnight cases for a hospital in Baltimore. But teleradiology doesn’t create new radiologists — it moves existing ones around. The global supply constraint remains.
Read faster. This is not a strategy. This is a stress response. Pressure to increase throughput without corresponding quality controls leads to exactly the fatigue-related errors described above.
None of these solutions address the fundamental imbalance: more scans, not enough readers.
Enter the second reader
Here’s what a second reader does in traditional radiology: a second set of trained eyes reviews the same study, independently, looking for findings that the primary reader may have missed. It’s the seatbelt of diagnostic imaging. Double reading has been standard practice in mammography screening for decades in many countries because it measurably reduces missed cancers.
The problem is obvious: if you don’t have enough radiologists for a single read, you certainly don’t have enough for two.
Unless the second reader doesn’t need to sleep, eat, take vacation, or get paid by the hour.
AI-assisted second reading is the most practical near-term answer to the diagnostic safety problem created by the workforce shortage. Not AI replacing radiologists. Not AI reading cases autonomously. AI as a tireless, consistent, always-available second pair of eyes that flags findings the primary reader may want to revisit.
What AI second reading looks like in practice
This isn’t science fiction. The technology exists today. Here’s how it works with MYAIRA AI:
1. The scan is acquired. A chest X-ray, for example. The DICOM image is sent to the PACS as usual.
2. AI analysis runs automatically. MYAIRA AI processes the image in under 3 seconds. It screens for 15+ chest and lung pathologies — pneumothorax, pleural effusion, consolidation, mass/nodule, cardiomegaly, and more.
3. Results are delivered alongside the image. The radiologist sees the original study plus AI-generated findings: confidence scores for each detected pathology, heatmap overlays showing the regions of interest, and a structured summary. No separate login. No extra window. The AI output lives where the radiologist already works.
4. The radiologist makes the diagnosis. Always. The AI doesn’t diagnose. It flags. It highlights. It says, “I see something here at 94% confidence — you may want to look more closely.” The radiologist uses their training, clinical context, and judgment to interpret the findings and write the report.
This is human-in-the-loop by design, not by compromise. The AI catches what fatigue misses. The radiologist provides the clinical reasoning that AI cannot.
Why skeptical radiologists should take a second look
If you’re a radiologist reading this with healthy skepticism, good. Skepticism is the right starting point. Here are the objections we hear most often, and honest answers:
“AI will replace me.” No. The shortage data makes the opposite case: there will be more work for radiologists in 2034 than there is today, not less. AI handles the screening layer so you can focus on the cases that require your expertise — complex findings, clinical correlation, patient communication, and procedural guidance. Radiologists who use AI tools will be more productive and less burned out than those who don’t, and that’s the competitive advantage.
“The accuracy isn’t there yet.” Fair question. Current chest X-ray AI systems, including MYAIRA’s, operate in the 94-97% sensitivity range for common pathologies on validated datasets. That’s not perfect. But consider the baseline: studies have shown that human reader sensitivity for subtle findings on chest X-rays ranges from 70-87%, depending on the pathology, reader experience, and reading conditions. AI doesn’t need to be perfect. It needs to catch the things that slip through when a radiologist is reading their 80th case of the day.
“I don’t want to be liable for AI mistakes.” AI-assisted analysis is explicitly positioned as a decision support tool, not an autonomous diagnostic system. You review the AI output. You write the report. You remain the physician of record. The AI is a tool in your workflow, like a CAD system in mammography — present, helpful, and ultimately advisory.
“It’s too expensive for my practice.” This is a real concern, and it’s one that most AI vendors have failed to address. Enterprise AI platforms with six-figure annual contracts and months-long integration projects are not accessible to a solo radiologist or a four-person group practice. That’s why MYAIRA offers a free tier: 50 AI analyses per month, no credit card required, no contract. Enough to test it on real cases in your own workflow before committing a dollar.
The accessibility problem
Here’s an uncomfortable truth about radiology AI in 2026: the practices that need it most have the least access to it.
Large academic medical centers and health systems can negotiate enterprise AI contracts. They have IT teams to manage PACS integration. They have budgets for innovation.
Solo radiologists, small group practices, rural imaging centers, and physicians in low-resource settings? They’re reading the same overwhelming case volumes with none of those resources. The shortage hits them hardest, and the existing AI market has largely ignored them.
This is a design choice, not an inevitability. Radiology AI software doesn’t have to cost $50,000 a year. It doesn’t have to require a six-month integration project. It doesn’t have to be sold only through enterprise sales teams. AI Bharata, the company behind MYAIRA, built its platform with this accessibility gap in mind.
MYAIRA AI is built for the 80% of radiology that happens outside large academic centers:
- Free tier: 50 analyses/month. No contract. No credit card.
- Professional tier: Unlimited analyses, PACS integration, priority support — at a price point designed for small practices, not hospital systems.
- Cloud-based: No on-premise hardware. No IT project. Upload or connect, and start analyzing.
- Self-serve onboarding: Sign up, upload a study, get results. Minutes to value, not months.
If you’re a radiologist in a three-person group reading 200 cases a day and wondering whether AI can help, the answer shouldn’t be “schedule a demo with our enterprise sales team.” The answer should be “try it right now, for free.”
From chest X-ray to everything
MYAIRA AI’s current capabilities are focused on chest X-ray — 15+ pathologies, sub-3-second analysis, confidence-scored results with heatmap overlays. Chest X-ray is the most commonly performed imaging study worldwide (over 2 billion annually) and the modality where AI-assisted second reading has the most immediate impact.
But chest X-ray is the starting point, not the destination. The platform is architected for multi-modality, multi-pathology analysis: CT, MRI, ultrasound, mammography, and pathology. The same workflow — upload, analyze, review — will extend across imaging types as capabilities expand.
AI Bharata’s vision is straightforward: every medical image, from every modality, in every setting, has access to an AI second reader. Not as a luxury. Not as an enterprise add-on. As a standard part of diagnostic imaging.
The second reader you can actually use
The radiologist shortage isn’t a problem that will solve itself. Training pipelines are too slow. Imaging volumes are too fast. And the consequences of the gap — delayed diagnoses, fatigued readers, missed findings — fall on patients.
AI-assisted second reading doesn’t fix the shortage. Nothing short of thousands of new radiologists will do that. But it addresses the most dangerous symptom: the diagnostic errors that occur when overworked readers are pushed past their cognitive limits.
A second reader that never tires. That processes in seconds. That catches what fatigue misses. That’s available to every radiologist, not just those at well-funded academic centers.
That’s not a threat to radiology. That’s a lifeline.
Watch: How AI assists radiologists as a tireless second reader
Ready to try AI-assisted second reading? Start with 50 free analyses — no contract, no credit card, no enterprise sales call. Or learn more about how MYAIRA AI works.