
From 33 to 1,000+: What the FDA AI Approval Explosion Means for Your Imaging Center
In 2016, the FDA had authorized exactly 33 AI-enabled medical devices. Total. Across all of medicine.
By mid-2026, that number exceeds 1,000 — and 77% of them are in radiology.
Read that again. More than three-quarters of all AI-enabled medical devices authorized by the FDA are designed to analyze, assist with, or augment diagnostic imaging. Radiology is not one of many fields being transformed by medical AI. It is the field. The laboratory where the entire medical AI experiment is being conducted at scale.
For imaging center administrators, radiology department heads, and practice managers, this creates a problem that didn’t exist five years ago. The question is no longer “Should we adopt AI?” It’s “Which AI, from which vendor, for which use case, governed by what framework, evaluated by what criteria, and integrated how?”
That’s a much harder question. And if you don’t answer it deliberately, the market will answer it for you — with sales pitches, conference demos, and competitive pressure that may not align with your patients’ needs or your practice’s realities.
The numbers behind the explosion
The FDA’s AI/ML-Enabled Medical Devices database tells a clear story:
- 2016: 33 total authorized AI/ML devices
- 2020: 160+
- 2022: 400+
- 2024: 700+
- 2026 (projected): 1,100+
The growth is not linear. It is accelerating. And within that growth, radiology dominates:
- Radiology/medical imaging: 77% of all AI-enabled device authorizations
- Cardiology: 11% (much of it imaging-adjacent — echocardiography, cardiac MRI)
- All other specialties combined: 12%
Within radiology, the distribution reveals market focus:
- Chest/lung applications lead, driven by chest X-ray AI, lung nodule detection on CT, and pulmonary embolism triage
- Mammography AI follows, with multiple FDA-cleared products for cancer detection and density assessment
- Neuroimaging (stroke detection, hemorrhage triage) represents a growing segment
- Musculoskeletal (fracture detection), abdominal (liver lesion characterization), and cardiovascular imaging round out the landscape
The practical implication: if you run an imaging center in 2026, there are likely dozens of FDA-authorized AI products relevant to your case mix. Not one or two. Dozens. Each with its own clinical claims, pricing model, integration requirements, and evidence base.
Why more options doesn’t mean easier decisions
The explosion of FDA-authorized AI products sounds like progress. And it is — scientifically. But for the people who actually have to choose, deploy, and govern these tools, more options create more complexity:
Overlapping claims. Multiple vendors offer chest X-ray AI that detects “15+ pathologies in under 3 seconds.” Multiple vendors offer lung nodule detection on CT. Multiple vendors offer mammography AI. The marketing language converges. The underlying technology, validation rigor, and post-market performance can diverge significantly.
Variable evidence quality. FDA authorization — typically through the 510(k) pathway for most radiology AI — establishes that a device is “substantially equivalent” to a predicate. It does not mean the device has been validated in a large-scale randomized controlled trial. Some products have robust clinical evidence. Some cleared with bench testing and small retrospective studies. The FDA pathway does not distinguish these for you.
Integration complexity. An FDA-cleared algorithm is a medical device. Integrating it into your clinical workflow — your PACS, your worklist, your reporting system — is an IT project. Some vendors offer seamless PACS integration. Some require standalone workstations. Some work through cloud APIs. The “clearance” does not tell you whether the product will actually fit into your reading room.
Cost opacity. Radiology AI pricing ranges from free tiers (like MYAIRA’s 50 analyses/month) to six-figure enterprise contracts. Per-study pricing, annual licensing, volume tiers, and bundled vs. modular pricing create an opaque market where comparing total cost of ownership across vendors requires significant effort.
Governance gaps. Who in your organization decides which AI tools to adopt? Who monitors their performance after deployment? Who is responsible when the AI flags a finding that the radiologist disagrees with? Most imaging centers don’t have answers to these questions because they’ve never needed them before. With 1,000+ products in the market, they need them now.
A practical evaluation framework
If you are responsible for AI adoption at an imaging center or radiology department, here is a framework for navigating the market. It is not exhaustive, but it covers the dimensions that matter most.
Clinical relevance: does it solve your problem?
Start with your case mix, not the vendor’s product catalog. What are the highest-volume studies in your practice? Where do your radiologists spend the most time? Where do the most errors occur?
A chest X-ray AI tool is valuable if chest X-rays are a significant portion of your volume. A lung nodule detection algorithm matters if you run a lung cancer screening program. A stroke detection AI matters if you’re a stroke-receiving facility. Match the tool to the clinical need, not the other way around.
Evidence quality: what has actually been proven?
Look beyond the FDA clearance letter. Ask for:
- Validation study details: How many cases? From how many sites? Were they prospective or retrospective? What was the reference standard?
- Sensitivity and specificity by pathology: Aggregate accuracy numbers hide variation. A tool that detects pneumothorax at 98% sensitivity but consolidation at 78% may not serve your clinical priorities.
- Subgroup performance: As we discussed in our post on AI bias, overall accuracy can mask disparities across demographic groups. Ask for performance data segmented by race, sex, age, and equipment type.
- Peer-reviewed publications: Is the evidence published in indexed journals, or only in vendor-sponsored white papers?
Workflow integration: will it actually get used?
The best AI algorithm in the world is worthless if your radiologists don’t use it. Evaluate:
- PACS integration: Does the product integrate with your existing PACS viewer, or does it require a separate window? As we explored in our burnout post, separate-window AI tools increase cognitive load and contribute to alert fatigue.
- Worklist integration: Can the AI triage findings and prioritize the worklist, or does it only produce results after the radiologist has already opened the study?
- Reporting integration: Do AI findings flow into the dictation workflow, or do they require manual transcription?
- Alert design: Does the product use intelligent alert thresholds, or does it flag every finding regardless of clinical significance?
Total cost of ownership: what does it really cost?
Calculate the full cost, not just the license fee:
- Software licensing: Per-study, annual, or volume-tiered?
- Integration costs: IT labor for PACS integration, testing, and validation
- Training costs: Radiologist training time, workflow adjustment period
- Maintenance: Updates, upgrades, support contracts
- Opportunity cost: Time spent evaluating and managing the tool vs. doing other things
Then weigh against the return: new CPT codes that reimburse AI-assisted analysis, reduced error rates, faster turnaround times, and radiologist satisfaction.
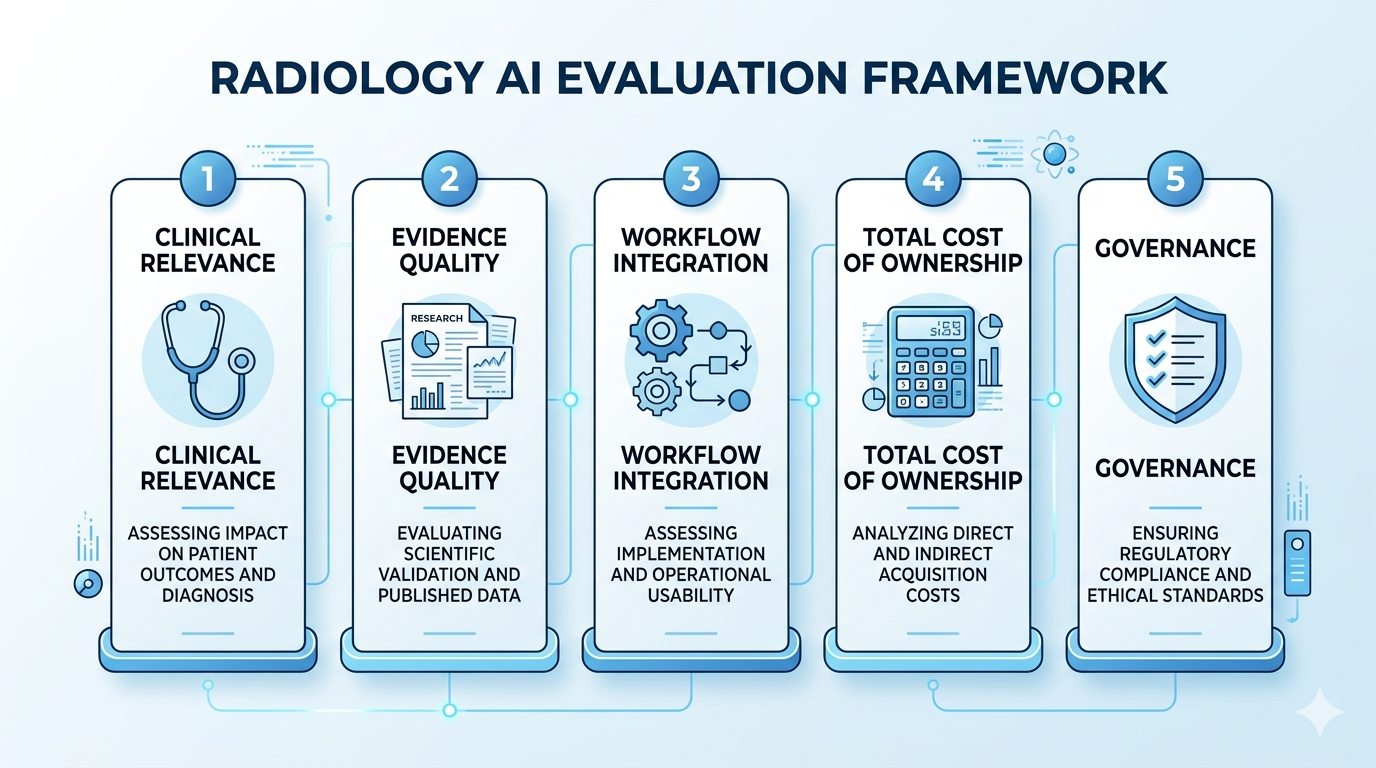
Governance: who is responsible?
This is the dimension most imaging centers overlook — and it may be the most important.
Establish an AI governance committee. This does not need to be a new bureaucracy. It needs to be a defined group — radiologist champion, IT lead, quality officer, practice administrator — that makes decisions about AI adoption, monitors performance, and handles incidents.
Define a review process. Before any AI tool goes live, it should pass through a structured review: clinical need assessment, evidence evaluation, integration testing, workflow pilot, and formal go/no-go decision.
Monitor post-deployment performance. An AI tool that performed well in the vendor’s validation study may perform differently in your clinical environment, with your equipment, your patient population, and your reading patterns. Track key metrics — sensitivity, specificity, false positive rate, radiologist override rate — on an ongoing basis.
Document everything. Malpractice liability in the AI era increasingly turns on documentation. What AI tools are in use? How were they validated? How are discrepancies between AI and radiologist handled? The imaging center that can answer these questions with clear documentation is in a much stronger position than one that cannot.
Where MYAIRA fits in the ecosystem
With 1,000+ FDA-authorized products, every vendor needs to explain why their tool deserves a place in your workflow. Here is what differentiates MYAIRA, built by AI Bharata:
Accessibility. Most radiology AI products target large hospital systems with enterprise budgets. MYAIRA is designed for the imaging centers and practices that represent the majority of radiology — small practices, outpatient centers, and facilities that don’t have a six-figure AI budget. A free tier with 50 analyses per month lets you evaluate on real cases before committing.
Friction-reducing design. We built MYAIRA around the principle that AI should reduce cognitive load, not add it. Sub-3-second analysis. Inline results. Confidence-scored, clinically filtered findings. No separate logins. No alert avalanche. The design philosophy we described in our burnout post is not marketing — it is the architecture.
Integrated sharing. MYAIRA is not just an analysis tool. Medixshare provides instant, encrypted scan sharing — the complete workflow from analysis to collaboration. When AI findings need to reach a specialist, they get there in seconds, not days. No CDs, no proprietary portals, no security vulnerabilities.
Transparent validation. We publish performance data across demographic subgroups. We welcome independent evaluation. We are aligned with EU AI Act requirements for bias documentation and training data transparency — not because we have to be, but because that’s what responsible medical AI requires.
The adoption window
The FDA AI approval explosion is not slowing down. If anything, the pace is accelerating as AI development tools improve and regulatory pathways mature. By 2028, the number of available radiology AI products will likely double again.
For imaging centers, the practical timeline is now:
2026-2027: Establish governance and pilot. If you don’t have an AI governance framework, build one. Select one or two high-impact use cases that match your case mix. Pilot with products that are easy to integrate and easy to evaluate.
2027-2028: Expand and optimize. Based on pilot results, expand AI usage to additional modalities and use cases. Optimize workflows based on radiologist feedback. Track ROI against new reimbursement codes.
2028+: Integrate across the imaging enterprise. AI becomes standard infrastructure, not a bolt-on experiment. Governance matures. Multi-algorithm management becomes a core IT competency.
The imaging centers that start this process now will have a two-year advantage over those that wait. In a market with a radiologist shortage that is only getting worse, that advantage translates directly into better patient care, better radiologist retention, and better financial performance.
The FDA has given the market over 1,000 options. The hard part is choosing wisely.
Ready to start your AI pilot? Try MYAIRA AI free — 50 analyses per month, sub-3-second results, zero integration complexity. Built for imaging centers that need answers, not enterprise sales cycles.
Need to modernize your image sharing? Get started with Medixshare — instant, encrypted sharing that eliminates CDs and proprietary portals. Free for patients and providers.